FROM WELFARE STATE TO SOCIAL STATE
Empowerment, Individual Responsibility and Effective Compassion
by Wilfried Prewo http://www.cne.org
About the Author
Wilfried Prewo is chief executive of the Hannover Chamber of
Industry and Commerce in Hannover, Germany, and a board
member of CNE. He is grateful to Michael Seitz of the
Hannover Chamber for his help.
INTRODUCTION
A little over a century ago, Bismarck pioneered the modern
welfare state. Pension, unemployment and health insurance
provided social and political stability in a new nation state,
kept socialism at bay and seemed to be the model for the
maturing industrial society. As workers were required to move
from job to job and region to region, and as the close bonds
between old and young generations within families became
looser, the welfare state replaced the old intra-family
generational contract with a societal contract. It was even
credited with initiating a virtuous cycle: For poorer parents, the
prospect of a pension made it unnecessary to rear many
children as a form of old age provision; instead, more could be
saved which, in turn, fuelled growth.
The cost of the welfare state was, initially, bearable. Benefits
were puny compared to today's. Incomes were growing, health
was improving thanks to leaps in innovation, and the pension
payments for a small number of retired people with still-low
life expectancies could easily be financed by a growing number
of young people soon to enter the labour force. The "age tree"
had its ideal, pyramidal shape.
The success of this model affordable, near-universal protection,
against Lord Beveridge's five evils (note 1) made us blind to its
basic design flaw. Whether in the forms shaped by Bismarck in
the 1880s, Roosevelt or Beveridge in the 1930s and 40s, the
welfare state treated the citizen as the recipient of an
entitlement bestowed on him and provided by government,
whether the latter was acting on a democratic mandate or, as in
Bismarck's case, as a benign autocratic patron.
With more and more generous benefits, politics whetted - but
did not sate - the appetite of a demanding electorate under the
quiet understanding that a major part of the cost could be
shifted to yet-to-be-born generations. The demographic trend
toward more and more old and fewer young people appeared
on the horizon, especially after World War II, but this time
bomb had a long fuse. Costs did rise substantially but did not
quickly bankrupt the system, since the predominantly national
economies were not exposed to severe foreign labour cost
competition, especially not from non-welfare state countries.
Increasing global competition has now exposed the Achilles
heel of the welfare state. In world markets, we no longer can
command prices that are generous enough to finance it. Jobs
are lost to more frugal countries. With higher unemployment,
the cost has become onerous. Finally, with an increasing
number of pensioners, the welfare state sucks up the savings
that we would urgently need as we leave the machine age and
have to invest and grow into the information age. The welfare
state is the albatross around our neck. We are now caught in a
vicious cycle.
Figure 1
There is no easy way out. While we can devise an efficient
social security system, a major difficulty in implementing it is
that, in the political arena, equity considerations take
precedence. Until recently, cutting benefits and costs was
practically not possible; where it happened, success often was
short-lived, with cut benefits soon reinstated via political
pressure. Now, the situation has changed; the notion that the
welfare state cannot be sustained finds increasing recognition.
However, this general awareness does not yet translate into
widespread support to cut specific benefits. The distributive
conflict, -who gains, who looses?- is not calming down, but is
heating up and is standing in the way of real reform. The
resulting reform paralysis is frustrating and can only be
resolved if efficiency and equity considerations are addressed
simultaneously.
Economically sound reform proposals will not always be of the
simple win-win-variety. The win-lose-situation is more likely,
in which this or that group's distributive status quo is
threatened, but the overall gain outweighs such partial losses.
If the reform proposals are promoted only by alluding to the
overall net gain and do not entail a compensation scheme for
the losers, they are brushed aside and, in the political debate,
dealt the fatal blow that they lack compassion for the socially
weak. To have any chance for a political hearing, reform
proposals must, at the outset, guarantee that everybody can
gain, that potential losses can be compensated. A revolutionary
system change must not be bloody.
In reconciling both efficiency and equity, the cornerstones of
this proposal are financial empowerment and individual
responsibility: To hand the individual the money required to
purchase the current level of benefits, and to leave it to him,
within bounds, whether he will do so. This will induce a
behavioural change because people will find it in their own
interest to economize on social security spending. While
guaranteeing that everybody can buy the current benefits, the
savings from restraint will be the consumer's to keep.
Preserving the no-loss rule is a basic tenet of the empowerment
model. This, together with the incentive to save, defines the
velvety characteristics of the system change. It must be politically
palatable, since it cannot be attacked for worsening
anybody's legitimate status quo (note 2)
This system change replaces the welfare state's top-down,
paternalistic and heady governance with a market solution,
which stands the social system on its feet, those of the
constituents. Individual behaviour is changed but the goal of
social safety is not called into doubt.
A market solution unlocks efficiency gains and makes benefits
more affordable. Elimination of waste helps to re-establish
societal consensus about the necessity of a social safety net. But
it will also make clear that, as a society, we can only afford a
social system which we stand ready to finance ourselves.
Gaming the system or shifting costs into future generations is
anything but socially responsible.
Back to contents
II. THE WELFARE STATE TRAP: LABOUR COST AND GLOBALISATION
Even with moderate growth, Western Europe is suffering from
record-high unemployment. Growth over the last three
decades has produced no or only few new jobs. This is in stark
contrast to the U.S., where the number of jobs rose by about 70
per cent from 1970 to 2002, while in Western Europe the increase
was less than 30 per cent over this period (Figure 2).
Unemployment will only recede, if labour costs can be lowered
significantly.
Since the 1960's, unemployment in Germany, the EU-country
we mostly refer to in this study, has been ratcheting upwards:
The additional unemployment generated during a recession
was, in the following upswing, hardly reduced, since the cost
structure was not corrected. Instead, labour cost kept increasing.
With the next recession, unemployment jumped again
(Figure 3).
While this relationship has been observed for some time, politicians
have closed their eyes and hoped that unemployment
would fade away in the next cycle. In fact, the long growth
period covering much of the 1980's saw some job creation also
in Europe, not exciting by U.S. standards, but very comfortable
relative to past European experience. The oil price shocks had
been accommodated and there was optimism that new service
industries would create more new jobs than would be lost in
the inevitable restructuring of old industries. On top of that,
the European Single Market brought new hope even for
stagnant industries.
On a global sphere and until the end of the 1980's, the main
markets and competitors of Western European companies were
in the triad of Western Europe - North America - Japan. China
and South East Asia were much talked about in the 1980's, but
were not yet a major investment location except for a few large
companies. Africa was totally out of the picture and South
America not yet back in.
In this situation, high European labour costs were, still in the
1980's, (barely) bearable, as labour cost premiums of up to 35
per cent within the triad could be partially compensated for by
productivity and other locational advantages; they were
usually not the deciding factor for investment decisions.
Consequently, successful European companies could remain
solidly embedded in their home markets, producing mostly
there and exporting from there. "Made in...." was a selling
point, be it "Germany" for cars and machine tools or "Italy" for
clothing.
With the melt-down of the Iron Curtain and the onset of the
information age, this situation has changed completely.
The labour cost benchmark is now set by emerging markets in
South East Asia and Central and Eastern Europe. These not
only offer low wages (many countries do) in the magnitude of
one tenth of European labour cost, but also productive labour.
They are attractive as production sites for labour-intensive
high-quality and, soon, high-tech products.
The exodus to these countries has begun. For Western
European firms, countries such as Slovakia or the Baltic
countries are the "Hong Kong around the corner"; they are
attractive for mid-size companies that, in the past, had not
considered going to far-away countries. As a result,
employment in Western Europe will stagnate or shrink further.
In post-Cold-War Europe, the increased competitive heat melts
the financial pillars of the welfare state. In the Bismarckian
variety of social security systems, financing is linked to
employment and, via payroll taxes that are partly borne by
employers, directly becomes a part of labour cost, regardless of
whether the covered risks are employment related or not;
examples are Germany, France, Belgium, and the Netherlands.
In the Beveridgean systems (examples are the U.K., Denmark
or Sweden), where social security such as a national health
system is financed out of government revenues, the costs do
not directly add to (indirect) labour cost, but the effect is eventually
the same: In the Bismarckian countries, payroll taxes
make jobs too expensive. In the Beveridgean countries, jobs are
eliminated as other taxes drive up gross wage demands and make the products too expensive on world markets. The main causes of sluggish job growth are the high cost of
labour, especially indirect labour cost (Figure 4) (note 3), and a large government sector (see again Figure 1).
In Germany, the archetypical Bismarckian welfare state that
can be used as a point of reference, indirect labour cost in
manufacturing industries amounts to 81,2 per cent of direct,
gross wages in 2001 (note4), which is about double the U.S. share.
Indirect labour costs in Germany have increased almost twice
as fast as gross wages since 1966, and this increase is closely
correlated with the rise in the unemployment rate (Figure 5).
Consequently, lowering indirect labour cost appears as a most
promising avenue to employment creation.
In 2004, the payroll taxes in Germany amount to: 19.5 per cent
of gross wages for pension insurance, an average of 14.3 per cent for health and 1.7 per cent for nursing (old age) care, 6.5 per cent for unemployment insurance: a total of over 41 per
cent of gross wages! Figure 6.
Half of this is paid by employers, adding to indirect labour cost
and making Germany the country with the second highest
labour cost, which for a German industrial worker was 22 per
cent higher than his American counterpart in 2002 (note 5) For the
German worker, his half of the payroll tax, together with his
taxes, reduces his take-home pay to 16 per cent below the American
level. Higher labour cost does not necessarily yield a
higher standard of living. Figure 7.
Consider this comparison: A German plumber has to work five
hours (at a net wage of Euro 8-9 per hour) to hire a painter for
one hour (at a cost of Euro 38-40 per hour) and vice versa.
Neither of them can afford that. Turning to do-it-yourself is
one reaction, though not a problem for society. But it is a
problem when the reaction takes the form that more and more
unemployed do actually not seek re-employment, instead
supplementing their unemployment benefits with black market
income and finding the combined to be higher than their
previous net wage. As a result, the welfare state is haemorrhaging. Fewer and
fewer actively employed people have to pay more and for more
social security recipients, raising labour cost even further and
adding to the job loss spiral.
On the investment side, the welfare state's consumption
spending drains resources needed for capital formation. In
1980, investment outlays still exceeded public welfare
expenditures in the major European countries; since then,
public social spending in these countries has exceeded
investment, and the gap has grown. (Figure 8). In the U.S., the
increase in the ratio of social spending has been far more
moderate, and is still dwarfed by investment.
The problem is exacerbated by demographic trends: In 1950,
Germany still had, with the exception of war-related
indentations, a population pyramid with a broad base of young
and a narrow cap of old people; by 2002, the "age tree" has
become a pumpkin with few young people, many mid-lifers
(still in the active labour force) and a growing, though not yet
dominant number of retirees. By 2040, it will resemble a mushroom:
very few young, few mid-lifers, many old people: The
pyramid will stand on its head! (Figure 9).
Under such conditions, pensions cannot be financed by a pay as-
you-go-scheme where the actively employed pay for the
pensions, health and nursing care of the elderly. By about 2030,
there will be about one pensioner for one active worker with
the consequence that the worker's pension payroll tax would,
on average, equal the average pension (note 6). Ask today's 25 yearolds
whether they believe that their children will be ready for
that. The "generational contract" underlying this system is an
unsustainable chain-letter. The only distinction from other
pyramid schemes - schemes that also portend to have a broad
and supportive pyramid base, but in fact are built on sand - is
that the pay-as-you-go pension system is legal, and the foulest
of all.
The welfare state impoverishes the current generation,
deprives future generations of growth opportunities, and even
shifts further liabilities onto a weakened future generation. As
well-intentioned as the welfare state's design may have been,
the results are perverse: Rather than guaranteeing social
security, it is now endangering it. The welfare state's fate will
mirror that of the equally morally corrupt and economically
exhausted socialist states at the end of the 1980's. Without
reform, it will implode just as Eastern Europe did in 1989.
Resisting such reform is the truly anti-social posture.
Back to contents
III. GOVERNMENT IS THE PROBLEM
The question is not whether but how - and, derived from that,
how much - social security is provided. This is where the
systemic flaw of the welfare state's social security systems
becomes apparent: Each is a uniform plan that disenfranchises
the individual. Benefits packages are standardized, one size fits
all. You cannot pick a lesser plan for a lower premium.
Consumer responsibility and choice have no material place; the
individual is bestowed with an entitlement determined by the
government, he is not a consumer/buyer of social insurance
products.
Social security plans are, by and large, not insurance systems.
The contribution or premium is not actuarially calculated.
Through the institutional tools of either the payroll tax or
outright socialization, individual consumption of social
security benefits is unrelated to individual expenditure. This
gives rise to moral hazard: The insured individual exploits the
system by extracting as many benefits as possible, since the
costs that he inflicts on the community of the insured are only
insignificantly borne by himself because premiums increase for
everybody. As more and more behave this way, the system
becomes grossly wasteful; worse yet, as prudent behaviour is
ridiculed, solidarity loses its moral base.
While any insurance is exposed to the moral hazard problem,
insurers try to eliminate or, at least, limit it with deductibles
and co-payments, differentiated premiums, incentives for
prudent use, or penalties for abuse.The welfare state, in contrast, invites moral hazard and makes itself hostage of entitlement mentality. The claims against the
entitlement system are never lowered, only raised, all the more
since claims can be conveniently filed at the voting booth.
Bowing to such pressure is not only costless to politicians;
those that are best at cheering on the electorate in its call for
more, the animators of the Club Med welfare state, can hope to
carry the grand prize of "taking care of people".
When business plans fail, they are scrapped or the firm goes
bankrupt. When government plans fail, they are expanded. In
attempting to control costs, the social security systems have
become increasingly politicised. Even those not run outright by
the government, but conceived as friendly workers' societies or
employer-employee partnerships under self-autonomy, have,
under increasing government intrusion, been converted to
government plans.
The welfare state's construct - how to provide social security -
answers, "how much? always more, but, in any case, the same
for everybody. While it is possible to stop the entitlement spiral
temporarily, there is no lasting success to such efforts:
Although German health care underwent many reforms, all of
them failed in their goal of redressing excessive health cost
inflation. They are the problem, not the cure.
Back to contents
IV. THE EMPOWERMENT REFORM
Breaking out of the welfare state's vicious cycle requires discarding the top down, social engineering approach of
government-run plans and organizing social security in a
bottom-up, consumer (incentive) driven way. Instead of
disenfranchising the individual, we must empower him to
evolve from a spoon-fed recipient of a uniform, one-size-fits-all
entitlement to a sovereign and picky buyer of social insurance
products, (note 8) while:
- enabling him to buy the current benefits,
- requiring him to buy only a minimum preventing the worst
case (becoming a welfare recipient), and
- allowing him to pocket any savings resulting from prudent
behaviour.
The empowerment reform, or "consumer model", contains five
elements:
Empowerment requires, first of all, purchasing power in
the hands of the individual that enables him to finance his
choice. But fresh money is not needed. All we have to do
is hand him the money currently spent on his behalf. This
preserves the no-loss rule.
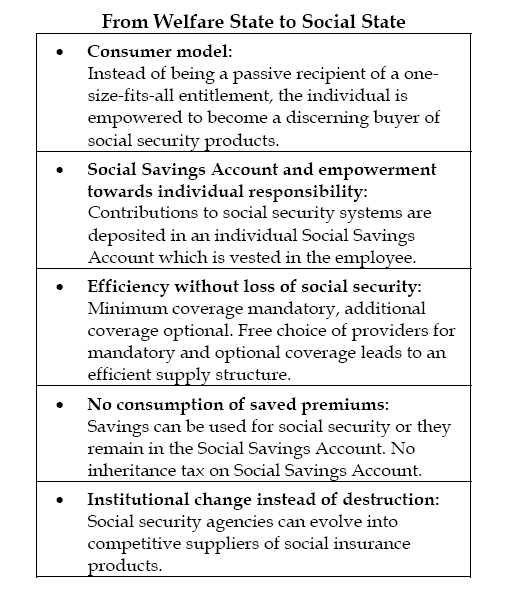
To this end, all current contributions to social security systems
should be deposited in an individual Social Savings Account
(SSA), which is established in the insured beneficiary's name.
In the Bismarckian systems, this means that the current
employer and employee payroll taxes are deposited in the SSA.
This transfer must be tax-free, to the extent that current employer
contributions are also tax-deductible. In the Beveridgean
countries where social systems are - partially or fully - financed
out of general tax revenues, the government must transfer the
corresponding monies into the SSA of the individual
beneficiary. In either case, the change is revenue neutral for the
government; it should not lose, either, but should also not get
additional revenues.
The individual SSA's must be corrected for current cross subsidies
or implicit solidarity transfers. For example, a health
insurance payroll tax, being dependent on salaries only, is not
an actuarially calculated premium. Lower income earners,
large families, pensioners, or women, each as a group, are
typically subsidized by high income earners, singles or unmarried
couples with two incomes and no children, the young, or
men.
Those belonging to the former group have a payroll tax
falling short of an actuarially calculated premium, while those
of the second group typically pay more (note 9). At this point, we do
not open a debate on the merits of current transfers, but,
strictly adhering to the no-loss rule, require that these transfers
are preserved: Consequently, the first group will have amounts
added to its own SSA deposits, the second group will have corresponding
amounts deducted; both will then have an SSA
balance that is sufficient to buy current benefits at full actuarial
value. Nobody - government, employers, employees - has been
made worse off
.-
Allowing the beneficiary to evolve from recipient to buyer
requires giving him the option of buying less (or more)
than current benefits and letting him pocket any savings
resulting from his choice. Instead of only making hollow appeals for prudent behaviour, the call for self-responsibility must be magnetised, if we want to hear an
echo. Whoever demands less should pay less.
There should be limits to choice. We may regret that, but
individual choice should have its limit where carelessness
would produce a welfare case. The community would not
gain, if an individual would not insure himself against
catastrophic illnesses in order to save on his premium and,
in the worst case, become a burden to society. But this also
defines an upper limit to mandatory coverage: It can be as
low as to prevent the welfare case. In the case of health
care, this implies, for example, mandatory coverage for
catastrophic illnesses and for ambulatory care beyond a
sizeable annual deductible. In the case of unemployment
insurance, mandatory coverage need not start on day one,
but, say, after six weeks of unemployment (note 10).
The individual, not a third party, controls his social
savings account deposit. He can use it to buy coverage for
the full current benefits or for as little as the mandatory
level. The premium savings in the latter case are a major
deterrent to "gaming the system". It is not necessary to
police socially unacceptable behaviour by bureaucratic
control, as is often suggested. The incentive of a lower
premium in the case of prudent behaviour is the best weapon
against moral hazard.
-
There is free choice among providers of health care,
unemployment, sick leave or pension insurance. Free
choice among providers applies not only to optional
coverage, but also to the mandatory part. Thus, mandatory
coverage does not mean government as the monopoly
provider. Analogous to mandatory automobile liability
insurance, where the insured can select among competing
insurers, free choice among providers will unlock a vastefficiency potential on the supply side. Moral hazard on
the demand side is, by far, not the only source of savings.
-
The premium savings resulting from less-than-full coverage
or from having chosen a more efficient provider will be
the individual's to keep. However, unspent balances
cannot be withdrawn for consumption purposes.11 The
individual can only draw on them either for expenses not
covered, e.g., a deductible, or for other social security
purposes, such as nursing care or additional old age
insurance. There can be wide latitude in defining social insurance,
allowing any investments deemed to secure social safety. This could include equity in a home or in a company. The reasons for proposing forced savings in the sense of
limiting the spending of SSA balances to social insurance
purposes are two-fold:
First, as the SSA balances build up
over time, the limits for mandatory coverage can be
lowered and become a variable depending on unspent
balances, thus increasing individual choice and incentives
to economize without the threat of becoming a welfare
case.
Second, the SSA addresses more than one area of social
insurance; in particular, we can and will need unspent
SSA balances, whether they come from less spending on
health care or other areas of social security, to build up a
fully funded pension system. While forced savings may
have a negative connotation to some, they do, in this case,
pave the way towards a market-oriented pension system.
Needless to say, being vested in the individual, unspent
SSA balances must, at the time of death, go to the holder's
estate, exempt from inheritance tax (note 13).
-
Finally, the Social Savings Account may be managed by
current social security administrations. There are
pragmatic reasons for this: We should allow the current
pension, health or unemployment administrations to seek a role in the new system. They and the sizable body of their employees would fight the new system, tooth and
nail, if we gave them no role and would just abolish them.
The German public health system (Gesetzliche
Krankenkassen) alone has about 150,000 administrative
employees (note 14), a formidable force; it is not necessary to make
enemies with them. We should give these institutions the
opportunity to also evolve into a competitive provider. If
they change successfully, all the better. However, there
must be no monopoly care-taker of the SSA. If an individual
sickness fund, for example, offers to manage the
account, it does so in competition with others. The
individual decides where he does his SSA banking. The
current system of monopoly care-takers of health, unemployment,
of pension insurance entails considerable
administrative overhead that can be saved by competition
among SSA portfolio managers.
In a nutshell:
1. Privatisation and efficiency on the demand and supply
sides.
2. Equity with the no-loss rule.
3. Safeguard.
First, the empowerment reform privatises the social systems,
unlocking the efficiency potentials that materialize in
privatisation schemes: Consumers gain from more choice and
economize by picking those services that appear optimal to
them on cost-benefit grounds; and on the supply side,
privatisation and competition bring better products faster to
market at the lowest price. Second, the no-loss rule assures
equity in providing everybody with the same incentives to act
prudently. Third, mandatory minimum insurance is the safeguard.
It should be added that the savings account proposed here is
not a novelty: It has been inspired by the Medisave accounts in
Singapore and related concepts that have been discussed and
experimented with in the U.S. since the early 1990fs . Archer
medical savings accounts (MSA), health reimbursement
arrangements (HRA), flexible spending accounts (FSA), and,
finally, the health savings accounts (HSA) that have been
established by the 2003 Medicare reform bill. Of these, HSAfs
appear to become a potent instrument toward consumer-driven
health care (note 15).
Back to contents
V. APPLICATION
The general criteria of the empowerment model need to be applied
to health, unemployment and pension insurance. It has to
be shown how features that are genuine to each of the three
areas can be embedded. In addition, the reform of current sick
leave payments is addressed: First, although the financing of
sick leave differs from the other three areas, it is related to
them, in particular to health insurance. Differences in the
duration and cost of sick leaves among countries, whose
societies enjoy a similar health status, highlight the importance
of institutional arrangements. Second, since employer paid sick
leave is typically limited to a month or so, even the most
drastic reform - abolishing it - would not slash the social safety
net. The argument that reform would threaten "social peace" is
ridiculous. Finally, the proposed sick leave reform is ideal in
showing the basic workings and strengths of the empowerment
model. Therefore, we address it before health reform with its
additional complexity of cross-subsidies or "solidarity
transfers".
As health reform is - and will remain - at the top of the social
policy agenda, it is dealt with in more detail. The contrast with
the increasingly politicised government health plans shows the
empowerment reform's ideological departure from the welfare
state's social engineering approach (note 16) and its promise in containing costs through its reliance on and respect for individual choice.
Critics of self-responsibility often argue that it would lead to
less than adequate preventive care. Such arguments do not rely
on logic, but usually dramatically allude to catastrophic
illnesses. The application of the empowerment model to
unemployment insurance shows that the opposite is likely to
happen: Given the right incentives, people will seek more jobtraining,
which is the best preventive care against
unemployment. Pension insurance is treated last, as here we
have to show how SSA balances can ease the - admittedly
burdensome - transition to a fully funded pension plan.
Welfare - aid to the poor - is not specifically addressed here,
not because reform is not urgent, but since its financing is not
related to employment and labour cost. The empowerment
reform would, however, substantially reduce the welfare
"problem": Easing the burden that the welfare state places on
labour cost would increase the take-home pay of low-wage earners
relative to welfare receipts. Second, welfare recipients
would not enjoy the monetary benefits entailed in the Social
Savings Account. Both aspects would make it more attractive
to leave welfare rolls and seek employment, while
concentrating society's resources on the poor that cannot be
integrated into the labour force.
Back to contents
51. Sick Leave
Typically, European employers are required to continue paying
employees that are on sick leave as much or nearly as much as
if they were working. The duration of employer-paid sick leave
is not open-ended, but limited to a period of, typically, a few
weeks to three months per incidence. After that, government or
health plans take over, often at a lower compensation level.
Employer-paid sick can amount up to 100 per cent (e.g.,
Germany); and it commences either on the first day
(corresponding to a zero deductible), as in Germany and Denmark, or after a waiting period of one to three days (e.g., 1 day in Belgium and Sweden, or 3 days in Italy or France),
during which the employee is "at risk" (note 17).
When, as in Germany's case, the employer pays 100 per cent of
income beginning with the first day of illness, the moral hazard
problem is most severe. As a result, about 4.2 per cent of
working days are lost to sick leaves in Germany, in contrast to
two per cent in the United States. (note 18) The cost to German industry
amounts to 3.9 per cent of direct wages (note 19). International
differences in sick leave, varying, as shown, by a factor of 2 or
3 - have little to do with the employees' health status (Figure
11).
- Figure 12 -
Gaming the system, or moral hazard evoked by full or near-full
compensation, is the plausible cause (note 20). Consequently, the cost
savings, or efficiency gains, from replacing the current system
with the empowerment model would be exceptionally large. In
keeping with the reform criteria, the reform steps would be:
-
Employers transfer an amount equalling as much as their
current sick leave expenses - in German industry, on
average, up to 3.9 per cent of direct wages - into the SSA of
the individual employee (note 21). In turn, the individual employee is then responsible to cover himself against income lost during sick leaves. A
pay-out corresponding to previous employer expenses is
sufficient to buy insurance at the current level of sick leave
benefits.
-
The individual is not required to cover all income losses of
sick leaves. The empowerment model only calls for
mandatory coverage at the level where uncovered income
losses would send the employee to seek public assistance.
Since only a few weeks (of currently employer-paid sick
leave) have to be covered, it is quite conceivable that there
would be no need for any mandatory sick-leave coverage
at all. Many people have some savings, and for those that
do not, their employer's deposit into their SSA would
build them up fast. However, granting that some minimum
coverage would be desirable even for such a limited
risk, mandatory insurance at the level of unemployment
coverage (around 60 per cent of net income) would
certainly suffice (note 22). Another option would be to start
mandatory coverage after a grace period of two weeks.
-
Sick leave insurance can be obtained from any insurer of
the beneficiary's choice. Private insurance companies can
offer sick leave insurance - they already do so, currently to
a clientele of self-employed. The public health system
(sickness funds) also could be a willing insurer; it has the
necessary actuarial information, as it processes the health
bills and already compensates income losses after employer-
paid sick leave runs out.
-
A policy with such co-payments (e.g., at a 60 per cent
compensation level instead of 100 per cent) or deductibles
(two unpaid weeks instead of coverage from day one)
would cost far less than currently. The savings would
remain in the SSA and could either compensate income
shortfalls in the case of illness or be used for other social
security purposes, such as building up a fully funded
pension plan. It does not take a clairvoyant to predict that, in countries with
above-normal sick leaves, their duration and cost would come
down to international benchmarks.
Sick leaves vary with leave benefits, as shown by an
international cross section in figure 13.
The Swedish experience is an interesting example, as it
highlights how, within the same country, behaviour (length of
sick leaves) changes when benefits are changed. In late 1987,
employer-paid sick leave was raised to 100 per cent (from 90%)
and started on day one (previously, the first day was not
compensated). As a result, sick leave in Sweden rose from 7.7
in 1986 to 9.7 per cent in 1988, its peak (Figure 14). In the wake
of Sweden's deep crisis, successive cutbacks were made in
1991, 1992 and 1993: the first day went unpaid again,
compensation was dropped to 75 per cent for the second and
third days, then 90 per cent for days 4 to 14. Concomitantly,
sick leave fell from its 1988 peak of 9.7 to 3.8 per cent in 1997.
With only one unpaid day of sick leave and with mandatory
benefits at 75 to 90 per cent, the Swedish reform policy of the
early 1990fs was certainly not asking for too much sacrifice.
Yet, these relatively mild corrections resulted in a 60 per cent
drop in sick leaves.
The reform movement was met with a political backlash, and
in the second half of the nineties, the pendulum in Sweden
swung back! Sick leave benefits were increased again and sick
leaves rose steadily to 6.1 per cent by 2002. This is a persuasive
example of the impact of government policies on the behaviour
of a rational citizen.
The Swedish case, however, is also an example of the obstacles
that such reform encounters. Although practically everybody
had to acknowledge that the previous sick-leave policy was
exemplary for the excesses with which Sweden's welfare state
had priced itself out of world markets, it took enormous political
energy to bring about even such moderate change.
Likewise, while everybody in Germany pays lip-service to lowering
indirect labour cost and many point to the current sickleave
policy as a prime candidate for overhaul, the suggestion
of minor changes - such as a drop in the compensation level to
80 per cent - immediately draws massive fire from the labour
unions (note 25). Cutting benefits, it appears, is only possible when
catastrophe strikes. Even a German unemployment rate of 10
per cent or more does not suffice as a wake-up call. When the
alarm bell rings, labour unions stuff it under the pillow,
admonishing us that waking up is a threat to social peace. As
absurd as that is, we must account for it. Therefore, the
entitlement reform compensates for a self-chosen drop in sickleave
benefits and makes, with financial incentives, reform
palatable. Neither government nor employers dictate a cut in
benefits in a top-down fashion. Benefits cuts are selected
voluntarily by the individual employee in return for a lower
premium, just as he decides to buy auto insurance with or
without a deductible.
Employers would gain, even if they transfer the full current
cost of sick leaves into the Social Savings Accounts of the employees:
With reduced absenteeism, machine utilization increases,
the cost of capital per unit of output decreases, and
additional costs of hiring replacement workers are saved (note 26).
More important, the past trend of the cost of sick leave would
be broken: During the period 1998 to 2002 alone, companies'
total costs for sickness have increased by 17.4 per cent (note 27).
During the same time, average income in Germany increased by 10.0
per cent (note 28); under the reform proposal, it would, in the future,
only increase at the rate of wages. Furthermore, both employers and employees would reap
health cost savings, since the documentation of sick leaves
requires a visit to the doctor's office.
Back to contents
52. Health
All European countries are exposed to excessive health cost inflation (Figure 15). This is, to a large part, unavoidable: Aging drives up health costs, and medical innovation comes at a price. But these are
costs that we are willing to bear. On the other hand, all national
health plans suffer from inefficiency; unnecessary costs are a
waste to society. In Germany, for example, the administrative
cost of the public health system has risen even faster than
medical expenses, although information technology and
standardized billing should have led to a decrease in the cost of
overhead.29 Instead, health care "reforms" have bloated administrative
expenses and posed disincentives to medical and
pharmaceutical innovation.
a. Health: The Problem
The core problem of a national health plan is that it is a plan.
The problem is not that we are planning - in this case,
providing for the prevention and treatment of illness. Every
day, we are formulating plans, what and how to work and how
we spend our time and money. Our plans are highly
differentiated: We may get up early or work late; we may
engage in sports or watch it from the couch. Everybody plans
individually according to his desires and circumstances.
The problem of national health plans is that each is a uniform
plan, one size fits all. Our shoes are different, fitting the size of
our feet, matching our clothing, or being suited for work,
dance, or sports. But our health plans are standardized. Not we
as individuals, but the government as our presumed agent
determines what is and what is not covered. Consumer
responsibility and choice have no material place. You cannot
pick a lesser plan for a lower premium, a higher deductible or
co-payment in exchange for a lower premium, or choose less
dental coverage than currently provided in exchange for other
options.
A system that does not reward restraint but disenfranchises the
individual, puts itself under permanent pressure: More and
more is demanded. Everybody tries to milk the system as much
as he can. Individual consumption is not related to individual
expenditure, neither in the Beveridgean system with its general
tax finance nor in the Bismarckian system with its payroll tax.
Beneficiaries behave like diners at an eat-as-much-as-you-can
restaurant: Each time we go there, we tend to eat too much. Afterwards,
we regret it.
On the supply side, doctors, dentists, pharmacists, and hospitals
do not compete for our, the customers', business, but render
their services. Their remuneration is dictated by cartels or
the government. More and more, government plans fix detailed
prices, prescribe services and formularies and subordinate
everybody under a budget.
Here the beneficiaries - there the providers, and each group
behaves like bears sitting around the honey pot. Everyone digs
in, grabbing with one hand as much as he can, while trying to
restrain the neighbour with the other hand. In astonishment,
politicians recognize that each time a fresh pot has been served,
it is gone in record time. Reform then first tries to appeal to
table manners in the form of round table talks or concerted
actions - with little avail; under the next reform the honey is
stretched and, finally, the contents are reduced by a false
bottom. Every time, however, the honey becomes more expensive.
And the ground rules remain the same: Everybody gets
the unitary brand and as much as he wants - as long as
supplies last.
We are still hesitant to discard this absurd plan with its foredoomed cost spiral and replace it with a variety of individual
plans. We are hesitant because we view health as a basic, elementary need. Everybody - rich or poor - should have access to health care. Nothing less than universal access to health care is suggested here. The fallacy is that we believe that health must be government
provided if it is to be available to all.
Clothing, housing and food also fill basic needs. We do not
want anyone, for reason of poverty, to be without clothes,
shelter or food. Yet clothing, housing and food are organized
differently from health care. We do not have the government
outfitter from which we obtain the one-size-fits-all coat. We do
not have the central quartermaster that provides standardized
housing. Nor do we eat the same menu in the people's canteen.
In the case of health care, however, (too) many still believe that
the goal - universal access to health care - requires a unitary
plan. Consequently, we do not speak of a health care market in
Europe, but of its provision. The insured are not purchasers,
customers and clients, but beneficiaries and "members" of
plans.
We did not have to lose any sleep over this as long as we spent
a small fraction of GDP on health care. But spending around a
tenth of national income on health should give cause to consider
whether, in a market economy, we should organize
health care as a market or ration it socialism-style.
Too frequently, we talk about the market economy as if it were
inconsistent with social policy and that the latter always requires
at least a good dose of socialism. This ideology has
drawn us deeper into the hole. Seemingly harmless
interventions were followed by more heavy-handed dictates
and, finally, formularies for drugs, fixed budgets, mandated
prices and fee schedules.
As many have said before: Social policy and a free market
economy are not contradictions. To the contrary, the efficient
and qualitatively best social policy is the one with a market
orientation.
b. Health: Reform Proposal
The proposal follows our guidelines and mirrors the reform
steps for sick leave benefits. In addition, the health care
proposal has to address the current cross subsidies between
different risk groups:
-
Each current beneficiary of a health plan receives - in the
form of a deposit in his Social Savings Account - the
money necessary to finance his current benefits (Figure
16). In turn, the individual himself is then responsible for
his health coverage, either by buying health insurance or
by contracting directly with a provider, be it a fee-forservice
physician or a managed care provider, such as a
health maintenance organization (note 30).
In the Beveridgean countries, the deposit into the
individual's SSA would come from the government which,
in turn, saves the corresponding amounts by
discontinuing to finance its current national health plan. In
the payroll tax-financed Bismarckian countries, the money
comes from the employees and their employers according
to their current shares in the payroll tax. In some
countries, such as in Germany, the payroll tax is shared
evenly by employers and employees; in others, such as in
France, Belgium, Italy, Spain, or Portugal, employers pay
a larger share.31 Of course, in mixed Beveridgean/
Bismarckian systems, money would come from
all three current financiers: government, employers and
employees. Furthermore, to the extent that current payroll
taxes are tax deductible - in particular, this holds for the
employers' shares -, contributions into the SSA must be
tax-free in order to preserve revenue neutrality.
In the Bismarckian countries, the payroll tax paid by an
employee and his employer is, except by coincidence, not
equal to full actuarial value of current benefits. It either
exceeds or falls short of that. Younger employees, singles,
dual income households with no children, higher income
earners32, and male employees tend to have a payroll tax
exceeding the full actuarial value of benefits.33
Correspondingly, the contribution (payroll tax) paid by or
on behalf of pensioners, households with only one income
and with dependents, low income earners, the
unemployed, or women tends to fall short of the full
actuarial value of their current benefits. This is especially
so for the elderly, large families and low income earners
(Figure 17).
For example, German retirees have health costs that are
much higher than those of the actively employed and their
co-insured. On the other hand, while they also contribute
to the health plans, the payroll tax rate is assessed, like for everybody else, only on their current income, their pensions, not on their previous salaries (note 34).
In 2002, the contributions on behalf of pensioners amounted to Euro 27.9
billion in Germany, while their health expenditures came
to Euro 63.4 billion, i.e., pensioners were subsidized to the
tune of Euro 35.5 billion or close to 60 per cent of their
costs. Underlying this subsidy is an implicit intergenerational
contract, analogous to that of the pension system itself (note 35). The subsidization of the elderly will become more severe as the proportion of senior citizens
increases.
Families with only one income and several dependents
constitute the other major group whose payroll tax falls
short of this group's health expenditures. In Germany, all
family dependents receive the same benefits as the payroll
tax-paying head of the household, whereas the payroll tax
is independent of family size. For every ten working employees
paying the payroll tax, there are 5.3 non-paying
dependents. Non-paying dependents had health expenditures
of Euro 18.9 billion in 2002.
With health expenditures unrelated to income, low income
earners also are subsidized; this also holds for the
unemployed. And women tend to have higher health expenditures
than men. In a pure Bismarckian system, where the health expenses
of all beneficiaries are financed by the payroll tax, these
subsidies are covered entirely within the system, by the
respective counterparts of young people, singles, high
income earners etc.
The empowerment model's no-loss rule requires that the
deposit into each SSA is at full actuarial value of current
benefits, i.e., it must suffice to buy the current full benefits
of each beneficiary, regardless of his and his employer's
contribution. Otherwise, the choices offered would not
unfold the same incentives for everybody. Therefore, the
payroll tax deposits into the SSA's have to be adjusted for
the current subsidies. Those with payroll taxes exceeding
the full actuarial value of current benefits will have
amounts deducted from their SSA's, while the others -
pensioners, families with dependents etc. - will have additional
amounts deposited into their individual SSA's.
No fresh money, however is required in this process, since
these withdrawals and deposits even out: Currently, this
cross-subsidization goes on "behind the scene", within the
sickness funds, but unobserved by the individual
beneficiary. All that would change is that we lift the
curtain and throw light on this process; the transfers
become explicitly and individually observable, as they
show up as credits or debits on the individual SSA's.
After the transfer, everybody will have an amount in his
SSA that is at full actuarial value of the benefits that he
currently enjoys. The no-loss rule is preserved. This is
critical for allowing the empowerment model to unfold its
economizing incentives.
In turn, the individual employee, having sufficient funds
in his SSA, is then required to cover himself against health risks.
The individual is, however, not required to buy a health
plan covering all current benefits. The mandatory or
minimum coverage would encompass those risks which, if
uninsured, could force him to seek welfare assistance and
become a burden to society. For the empowerment model
to unfold its strength, it is also not necessary to limit
mandatory coverage to absolute bare-bones essentials. A
comfortable level of mandatory coverage, with the right
structure of deductibles and co-payments, would already
provide significant incentives for prudent use of health
care. It is, therefore, not necessary to engage in a debate of
what is exactly the lowest possible mandatory coverage,
below which the welfare risk is imminent. We can be generous
and, rather, err on the high side.
In the case of health care, coverage of catastrophic
illnesses would, of course, be mandatory. Most treatments
requiring hospital stays would be included, possibly with
a co-payment or deductible. Chronic illnesses requiring
continuous or frequent treatment would be likewise
covered. In the case of outpatient medical treatment,
mandatory coverage could begin after a fixed annual
deductible or a thirty per cent co-payment. Also, the
aggregate of all annual co-payments and deductibles
would be capped, for example, at 4000.00 Euro. Putting an
upper limit on the total of annual risk sharing is a backstop
guarantee that the beneficiary is absolutely safe from
falling through the net. On the other hand, aside from new
co-payments and deductibles, the mandatory package
would not include medical expenses that, even if currently
covered, can be borne by the individual. Examples are eye
glasses or dental care.
-
There is free choice of health care providers. Only the extent
of mandatory coverage is prescribed. Provider and form of
that coverage are up to the individual to choose. The
provider need not be an insurance company, but could
also be a health maintenance organization or a preferred
provider network. The individual may choose a fee-forservice
plan that allows him to see any doctor of his choice
or he may subject himself to restrictions that might come
with managed care. Of course, these plans will have
different costs. The respective premium savings are a
strong incentive to "shop" for the best plan. What is "best"
is determined by the individual, not by politicians or
bureaucrats (note 36).
Beyond mandatory coverage, both scope of coverage and
providers are optional. The individual may, with his SSA
deposit, buy the current benefits or as little as the
mandatory level. And he can buy benefits that are
currently not covered if he realizes savings in other areas.
-
Any savings will belong to the individual and stay in his
SSA. Premium savings come from two sources, from
choosing either less coverage than currently provided or a
less costly provider. The individual can use his SSA
balance to pay (self-insure) health care expenses that he
has not covered (for example, eye glasses or a copayment),
or he can use the SSA balance and invest in a
retirement fund or other instruments raising his social
security.37 The savings resulting from prudent behaviour
in the areas of sick leave, health care or unemployment
insurance can ideally be used for building up a fully
funded pension plan.
-
As there is free choice of providers and plans, the individual
is also free to choose his SSA fund manager. No qualified
institution should be excluded from offering its services as
an SSA manager. The current government health plans or the legally mandated sickness funds may also offer to manage the individual SSA's. It is quite conceivable that
they will not be shunned by the individual. For, in a
market environment, these previous bureaucracies will
quickly change, just as mail and telecom providers did
change with privatisation. Sickness funds even have a
distinct advantage over new private SSA managers: Currently,
they account for all of the cross-subsidies between
old and young, rich and poor. This information gives them
head-start opportunities compared with other providers.
The question is whether they take a defensive attitude and
try to resist change or whether they view it as an
opportunity. We should leave that decision - and its
consequences - up to them.
c. Health: Quality and Price
The empowerment model improves health care and reduces its
cost. Since everybody may choose his provider - insurance or
capitation-based HMO, fee-for-service plan or managed care -
everybody gets a plan that, in his view, not some politician's,
serves him best. And since beyond mandatory coverage
everyone can determine the extent of coverage, he will spend
the money in those areas that he desires. Value is in the eye of
the beholder. Nobody has to pay for a plan or for extra
coverage that he does not want.
Using our analogy again: We replace the fixed-price, unitary
food-plan, monopoly eatery with highly varied, fiercely
competing restaurants. There are those with table cloths, flower
arrangements and extensive wine lists; and there are the family
restaurants, the chains, and the serve-yourself cafeterias.
Instead of a unitary diet, each restaurant allows the customer to
choose from an exhaustive menu and compose his own order.
Only a minimum diet (mandatory coverage) is prescribed. The previous unitary plan is also included in the offering, at no more than its previous cost. Which restaurant arrangement
would you prefer?
Whatever level of quality we choose, it will become available at
least cost, since everyone will try to preserve his - his own and
valued - SSA balances and spend only as much as necessary.
Since different plans come at different costs, with more
expensive plans leaving less to be added to his SSA, he will
contract only with such providers whose services he values at
least as much as their cost. Waste which was caused by careless
(not cost-conscious) use will be eliminated, since, with a
deductible or co-pay, services are no longer perceived to be
free.
Imprudent individual behaviour is no longer externalised,
shifted onto the community of all beneficiaries. Unnecessary
visits to doctors would vanish. A patient would not embark on
an odyssey visiting specialist after specialist without regard for
cost, but will consider the cost of duplicate exams and lab tests.
He will ask his doctor and, first of all, himself, whether he has
to return for a follow-up visit after his nose stops running. He
will no longer ask the doctor to give him a sick leave slip for a
week, when his tennis elbow aches on Monday morning.38 Selfpayment
of small bills that fall under a deductible would relieve
the insurer of substantial administrative cost; hence, the
premium cutback would be more than the actuarial value of
the deductible. Likewise, an insurer could offer the beneficiary
to submit bills for reimbursement only quarterly or semi-annually,
or when the total has exceeded a set amount, with
respective premium savings passed on to the individual (note 39).
On the supply side, consumer choice would, above all, bring
about an efficient and competitive structure: Benefits and
prices will be market-determined, not bureaucratically dictated
or negotiated between supplier and provider cartels. Health
care will no longer be structured along guild-like professional
or corporatist rules. Why should, for example, the fee-for
service physician practice be the only or dominant form of
providing ambulatory care? Cost decreases can be achieved in
a service-industry: Health maintenance organizations or
preferred provider organizations will be offered to and chosen
- or rejected - by the individual. The fee-for-service practice will
not disappear, but each form of service will carry its price tag.
We will have a variety of plans fitting a variety of individual
needs. Again, we do not prescribe, but let the individual
choose his preferred option (and pay or save accordingly).
d. Health: Competition and Supply Structure
For outpatient care so far, Germans see only a fee-for-service,
often solo-practicing, physician. Hospitals are, typically, owned
and operated by communities or charities. Doctors in private
practice cannot operate in hospitals; ambulatory care by
doctors in private practice and stationary care by hospitals are
separated, with each side guarding its turf. As of 2004 hospitals
may also treat patients on an outpatient basis. Ownership of a
pharmacy was until 2004 limited to one per pharmacist. Now, a
pharmacist may own up to four pharmacies. Legal and
professional regulations, some of them rooted in guild-like
structures had prohibited multi-specialty group practices,
chain or mail-order pharmacies. State control over opening or
expanding a hospital allowed little room for private hospitals (note 40).
As a consequence, HMO's are still unknown, preferred
provider networks do not exist, there are no pharmaceutical
benefit managers, no physician practice-management
companies41, while in other countries, above all in the U.S.,
there has been rapid structural change and experimentation
with new organizational forms over the last two decades.
It would not be necessary to have the government promote
new forms of service. All we would have to do is allow them:
Give people free choice of providers and lift restrictive
regulations. Structural change would follow immediately, especially when cost savings from alternative forms of service and a variety of health plans become apparent.
Consumer choice means supplier competition. Today, doctors
and hospitals spend an inordinate amount of energy on how to
extract remuneration out of the public health systems. In the
empowerment model, they will compete for the patient's
business and strive to offer alternative, better or less expensive
services.
The empowerment model emphasizes choice instead of the
imposition of a unitary form of service. Therefore, we do not
take sides - for or against managed care, for or against
traditional pharmacies, for or against public hospitals, for or
against fee-for-service-practices, for or against physician
practice-management companies. We leave this choice up to
the consumer. Different plans entail advantages or
disadvantages for the individual and will come at different
prices.
Overall, health care costs may or may not absolutely decrease,
as aging and technological advances tend to push costs up. But
whatever total costs we will have, they will be at the minimum
for the level of care desired by society and markedly below the
cost trend of the current system.
e. Health: Criticism and Objections to reform proposals
The empowerment model finally puts the patient, as a
consumer, on a level playing field with the suppliers (doctors,
hospitals, insurers, managed care providers). Critics are quick
in raising objections:
- (i) Patients lack medical information to make sound
judgments. Patients are, in most cases, not medical experts. Granted. Do
you have to be an automotive engineer or a computer expert when buying a family car or a home computer? When the car breaks down, we get it repaired; we do not need to self diagnose
the problem and prescribe the repair (therapy). We order the outcome ("get it fixed"). We know from our own or others' experience where we get the best service, whom we can
trust, where we get our money's worth. Sometimes we make the wrong choice and are disappointed.
We will remember and not repeat that mistake. The parallel to health care is obvious. Not possessing the same information as a medical expert, seemingly puts us at a
disadvantage. But in the empowerment model, our distinct
advantage is that we can take our business elsewhere, and
advise our friends likewise. Competition and freedom of choice
of supplier forces the latter to always try to use his best
judgment and, together with the looming threat of liability, do
anything to prevent malpractice. There is no guarantee that we
always receive the best service. But, overall, such a system
minimizes bad calls.
- (ii) Patients are not mature.
There are many critics that hold the individual not mature
enough to be a wise shopper of health services, when offered
the option of a sizeable deductible, even when limited by an
annual cap of about 4.000 Euro, as suggested here. This is
grotesque. Each owner of a car bears the cost of a tune-up, an
inspection, tires, and depreciation. These costs easily add up to
4.000 Euro annually. We certainly hold every car owner, rich or
poor, responsible for these costs. Imagine how we would drive
if our auto insurance would pay for burnt-up engines or wornout
tires. We even hold the individual mature enough to buy a car and
decide all by himself whether he wants to buy, on top of
mandatory liability coverage, collision insurance for self inflicted damage to his car. For the smallest new car, this is a risk of 10.000 Euro.
We also entrust our citizens to decide on their own whether
they want to marry and have children - decisions that do not
only have grave financial consequences. It is, indeed, grotesque
to claim that an individual is not competent to decide about a
4.000 Euro deductible. Strangely enough, those that contend so,
will say that they themselves, of course, could make such a
decision. The guardians of the welfare state lose their elite
status when the troops become smart.
- (iii) People will save themselves sick.
In striving to save money and increase his SSA balances, the
individual would, critics claim, cut down on necessary medical
services. This is a serious argument. But there are ways to prevent
a prudent consumer from skimping on necessary
purchases. First, the forced savings concept of the SSA prevents
the individual from using his SSA balances for a vacation or a
car purchase. Second, deductibles and co-payments can be
structured in such a way that they offer incentives for
preventive care. For example, there are insurers which waive
the deductible if the patient has had his routine check-up.
Finally, preventive care that is related to catastrophic illnesses
can be included in the mandatory package.
- (iv) Young people will underinsure themselves.
Young and healthy people may restrict themselves to the
mandatory package and buy a frugal plan. When they get
older, they may realize, with regret, that switching to a more
extensive and comfortable plan is very expensive, since
actuarial rates will then be much higher.
This argument is valid, but where is the problem? Those that
decided on a minimum plan in their earlier years have saved a lot. Their SSA balances allow them, as they become older, to step up to a more expensive plan or to cover extra benefits out
of their balances. Or they have, instead of additional health
coverage, bought more life insurance or used their SSA
balances to invest in a house or other assets on which they can
fall back, if necessary. And to repeat: The minimum mandatory
coverage is the back-stop that prevents a drop to welfare levels.
- (v) Optional coverage has no effect on hospital expenses.
Tertiary illnesses - such as cancer or stroke - would be included
in the mandatory package. Hospital care takes the largest slice
of the health cost pie - in Germany 32.1 per cent (2002).42 If
hospital care is in the mandatory package, how would the
empowerment reform save money in this important area?
In the case of hospital care, there is relatively little moral hazard
on the demand side; a deductible makes little sense here:
Nobody - with or without a deductible - wants to undergo
unnecessary surgery or stay in the hospital for excessive
periods. There is, however, considerable waste on the supply side. In a
competitive system, such as among U.S. hospitals, hospital
stays have been shortened tremendously. In the noncompetitive
public health systems of Europe, hospital stays are
being shortened now, but the trend has set in much more
slowly and we are still far behind U.S. benchmarks. In Europe,
there are more hospital beds and hospitalisation occurs more
frequently and the average stay is longer than in the U.S.: The
average stay for acute care in the U.S. has been 5.7 days as
compared to 11.6 in Germany or 9.2 in Switzerland (Table 2).
The German public health system has, until 2004, reimbursed
hospitals for the length of a patient's stay, irrespective of
treatment. Depending on the type of hospital - general care in a
rural region or teaching hospital in a city - a day was billed on
average at somewhere about 320 Euro. Per-diem reimbursement
have tended to lengthen hospital stays: In order to break even,
a patient was kept longer than necessary. Consequently,
hospitals had little incentive to optimize. To the contrary: if
they decreased their cost, their per-diem was reduced; if they
raised their cost, they documented it and tried to get an increase in their per-diem reimbursement.
As of 2004, remuneration is DRG43 based. The change was announced
already three years before; therefore, hospitals had adequate
time to prepare and have already slashed hospital stays before
the change took effect in the beginning of 2004.
With empowerment reform, choice of suppliers means that
hospitals will compete for the patient's business. Rather than
banding together in hospital associations and trying to extract
reimbursement increases from the sickness funds, they will
address the patient (or his insurance company as his agent).
They will form voluntary alliances with other hospitals, merge,
and outsource. The strict separation of ambulatory care by feefor-
service physicians from stationary care by hospitals and
their doctors will be replaced by flexible cooperation dictated
by cost advantages. In trying to bring costs down, hospitals
and doctors will make better use of information services. Public
hospitals will no longer be run by politicians and their appointees.
Auto liability provides a good analogy: It is mandatory as well,
but there is free choice of insurers. Competition among them is
stiff. Some of them would prefer a cartel-like setting where
they add up their cost, present it to a regulatory body and
negotiate rates. Free choice of liability insurers, diversity of
plans, bonuses and rebates for safe drivers have kept rates at a
competitive minimum.
Likewise, cost savings from opening hospital care to competition
will be large, just because hospital care currently takes the
largest slice of the cost pie and the bureaucratic system entails
so much dead weight loss. None of these cost savings must
come at the price of reduced quality. To the contrary, competition
always provides the impetus to improve.
53. UNEMPLOYMENT
Insurers differentiate their premium structure according to risk
categories, in order to induce prudent behaviour and reduce insurance
claims to a minimum. Auto liability insurance is a
good example for unemployment insurance, where everybody
is also required to be covered. Yet, in the case of auto liability
insurance, nobody demands that everyone should pay the
same premium, no matter how often he causes an accident. On
the contrary, the rebate system, which gives discounts to
accident-free car owners, is considered fair. The discount is
determined by the frequency of accidents, i.e., the number of
insurance claims, over the past years. If all car owners were
charged the same premium, the incentive to exercise caution
would be considerably lower. Premium differentiation leads to
fewer insurance claims, fewer accidents, and higher premium
savings.
Unemployment insurance, as we know it in Europe, disregards
this potential for premium savings. The unemployment payroll
tax rate, being the same for all, implicitly assumes that the
individual, through his own behaviour, cannot influence the
risk of losing his job. True, we cannot fault an employee for
every job loss; his employer may lay him off for reasons
unconnected to individual work performance. Consequently,
employers pay a share of the unemployment premium or
payroll tax: in Italy, employers pay nearly all (4.41 of 4.71%); in
Germany, they pay half (of 6.5%); in the Netherlands, they pay
less than employees (1.55 of 7.35%) (note 44).
In June 2003, 34 per cent of unemployed Germans had a new
job within three months45, suggesting that some of the
unemployed became so voluntarily, having first given up their
old job before looking for a new one. In Germany,
unemployment compensation begins immediately, on day one
and at a level of 60 per cent of net income for those without and 67 per cent for those with children; the unemployed do not pay the payroll tax for health or pension insurance, but continue to enjoy all benefits. Consequently, the difference between the
take-home pay of a low-income worker is not much higher
than unemployment compensation (note 46).
If the unemployment payroll tax were differentiated, i.e., lower for those that accept
an unpaid grace period of six weeks, socially beneficial
behaviour would be rewarded: Those that look for a new job
would do so while still employed. Total unemployment would
be lower, unemployment outlays would decline, making society-
at-large better off; and, with a lower unemployment
payroll tax, labour cost will decline and jobs will be more
competitive.
Training and education have a distinct effect on unemployment.
With its vocational training system, Germany is a
good example. (The experiences of Austria, Denmark, or
Switzerland, all having vocational training systems, are
similar.) Few employees in Germany . 13.8 per cent of the
labour force - are unskilled, having no vocational training or
academic degree; yet they make up more than one third of the
unemployed (note 47) and their unemployment is twice the average
unemployment rate. On the other hand, those with vocational
training, e.g., an industrial mechanic, have an unemployment
risk 13 per cent lower than the average (note 48). (Figure 18).
Training is the best unemployment insurance (note 49). Why not reward those that undergo training with a lower
unemployment premium? It is justified on individual actuarial
considerations. And it is called for on social grounds, since
society could be spared many negative effects that come with
unemployment.
Training is also the best policy against youth unemployment.
Countries with vocational training systems solve the school-towork
transition problem. Such countries - Germany, Denmark,
Austria, Switzerland - tend to have relatively low youth
unemployment (Figure 19).
In turn, in countries without vocational training, youth
unemployment rates may even exceed 20 per cent (Spain,
France, Italy). As youth unemployment often lies at the root of
criminal behaviour, youth training yields a win-win-situation
for individual and society. Why not make youth training attractive with the prospect of a lower, actuarially warranted unemployment premium?
Furthermore, rebates and bonuses could be considered for
those that have a good employment record, similar to auto
insurance for drivers with an accident-free history. Whoever
has been employed for a long time period, may not just have
had plain luck, but often his attitude and efforts - such as
further training - have made his job safe.
The empowerment model is ideal for incorporating these
features:
- (1) Each worker receives - in the form of a deposit in his Social
Savings Account - the money necessary to finance (insure)
his current benefits. In the Bismarckian countries, the
employer and employee shares of the unemployment
payroll tax (in Germany, each side pays 50% of a payroll
tax of 6.5%) would be put into the SSA. In the Beveridgean
countries, the money would come from the government's
current tax sources (Figure 20). In turn, the employee is
required to finance his unemployment insurance. He is
able to buy the current benefits.
- (2) The employee is, however, not required to buy
unemployment insurance according to current benefits.
Mandatory or minimum coverage would be at least as
high as welfare support. Beyond that, coverage would be
optional. Also, coverage would not have to start from day
one, but, say, after six weeks in order to minimize search
unemployment and entice people to start looking for a
new job while still employed. The unemployment payroll
tax would be differentiated according to training, i.e., risk
categories.50 Likewise, bonuses reflecting the employment
record would be offered.
- (3) In such a system, there is little reason for a monopoly
unemployment agency. Unemployment coverage could be
offered by any willing insurer. The beneficial effect would
be that competing insurers will take an immense interest
in job counselling. While that is currently done by
government unemployment agencies, anecdotes about
their inefficiency are over-abundant.
- (4) Any premium savings below the current payroll tax will be
the employee's to keep and will augment his SSA balance.
The employee can withdraw from it in case of
unemployment or he can use it for other social security
purposes. Premium savings from sick leave and
unemployment will probably be the major sources for
building up a fully funded pension plan.
- (5) Again, the fifth criterion is that the individual is free to
choose his SSA fund manager.
As with health or sick leave, the empowerment model
transforms the individual into a critical buyer. In the case of
unemployment insurance, he will, especially, be critical of
spending that is not insurance related. In many countries,
governments have shifted make-work programs and other
costly labour market policies onto their unemployment
agencies. While these receive government funds in carrying out
these mandates, they are usually underfunded, implying that
the employees, without having been asked, must subsidise the
remainder with their payroll taxes.
To the extent that only those that pay into unemployment
insurance are the beneficiaries of these labour market policies,
the subsidies may be justified. But since anybody in society
may be a beneficiary, it is unjustified to impose the cost on the
employees and their employers alone. The empowerment
reform would lead to a demand by the insured employees that
others also pay their share, i.e., that such labour market policies
are fully paid out of general government revenues. This will
lead to an honest discussion of the merits of such policies. In
Germany, approximately 40 per cent of the unemployment
agency's expenditures are for non-unemployment
compensation, i.e., labor market policies. In 2003, the
government paid about 11 per cent (6.2 billion Euro) of the
unemployment agency's budget (57 billion Euro)(note 51). In a fair system, the unemployment payroll tax would be 4 rather than
6.5 per cent.
Back to contents
54. PENSION REFORM
a. PENSION REFORM: The Problem: The Generational Contract
Old age provision typically comes from three sources:
mandatory government pension plans, company retirement
plans, or voluntary, individual old age provisions (Figure 21).
In most Western countries the mandatory government pension
plan dwarfs the two other provisions. The mandatory old age pension plans of the welfare states are financed in a pay-as-you-go system. It is based on the
"generational contract", according to which the currently active
employees pay for the pensions of the elderly and also raise the
future generation, on the tacit understanding that the future
generation will pay the pensions of the active generation, once
it reaches retirement.
The generational contract is a euphemism of unrivalled
cosmetic camouflage: There is no contract spelling out a
binding formula with individual responsibilities firmly tied to
benefits; one contracting party is not yet alive or has not yet
grown up; and the actively employed may violate the contract
with impunity - by not generating the offspring as the payers
of the future.
We speak of social "security" and old age "insurance". This is a
dangerous misnomer. Our language affects our thinking and
we believe that the pension system is, indeed, insurance. But the
pay-as-you-go system provides today's money only for today's
elderly (yesterday's workers) in return for their previous efforts
in raising the active generation. The active generation does not
provide for its own future pension. Only that could be called
insurance; it could take either of two forms,
- capital formation: with extra savings we can build up a fully
funded pension plan which we then draw down in
retirement; or
- human capital formation: raising children that will support
us.
Financially, our mandatory pension systems have either no or
insufficient funds to cover future pension claims.52
Demographically, we have broken the generational contract by
no longer raising enough children as the alternative to a
capital-funded plan.
The generational contract is a chain-letter, being sent by the
pensioner to several actively employed, asking them to jointly
share his pension payment. The letter concludes with the
advice to generate a sufficient number of children, raise and
educate them so that, when the parent generation is about to
retire, it will have a sufficient number of addresses to mail
similar letters to. If that advice were strictly adhered to, we
could call this old age provision or insurance. It is but a
pyramid scheme.
In a chain-letter, no letter writer can hold his addressees liable
for his claim. Those that have raised children do not get a
higher pension than those that did not, to the contrary: Women
may get some pension credit for raising children, but in any
case less than when they forego children for work. Consequently,
the insurance notion of old age provision - raising an
adequate future generation - is fully discredited.
Pyramids are built on sand. As the parent generation has failed
to generate enough children, it realizes that it has cut off the
branch on which it is sitting and has become a victim of
insurance illusion. Nonetheless, as this generation retires, all
members expect full benefits; looking for Ersatz support, they
turn to the state and take it hostage as the presumed guarantor
of the pyramid scheme. The ploy works, since with fewer active
people, the pensioners will have sufficient voting power.
Bismarck did not plan it this way, but neither was he a fan of
universal suffrage.
In defence of the pay-as-you-go pension system, its supporters
invoke solidarity. Nothing could be further from the truth.
Solidarity asks society to stand shoulder to shoulder, with the
strong supporting the weak, to the extent that the latter cannot
help themselves. Solidarity also entails a quid pro quo: If the
present generation expects the support of the future generation,
it first has to do its best to raise the offspring to the necessary
strength. But, having failed that, it usurps its voting power by
taking out an onerous mortgage on a numerically weak future
generation and assigning government as the trustee to this
selfish scheme. Politicians find it to their gain to endorse and
sanction this antithesis to solidarity. With such hypocritical
abuse of the concept of solidarity, it is no wonder that the
young respond with cynicism and even give the cold shoulder
to those that legitimately need compassion.
The major fault is not that future generations are not being
asked whether they want to "sign" the contract: Born into a
society, we have to assume many responsibilities imposed and
already assumed by generations ahead of us; in turn, we also
receive, as a gift, the hard- and software, infrastructure and
culture, that earlier generations have left behind. If we do not
like the dowry, we can emigrate.
The major fault is that the active generation can uphold its
claim of future pension receipts in full conscience of the fact
that it has not sufficiently raised children and invested in their
human capital. We do not want to hear that.
When Bismarck introduced pension insurance in 1889, the
generational contract posed no imminent problem. There were
many children, more than the actively employed, and there
was a tiny number of elderly that could claim benefits, as life
expectancy was about 45. Consequently, the age pyramid had a
broad base and it was not high. Pension reform had the effect
of lowering the birth rate, desirable at that time.
Of course, a fully funded pension system would, even at that
time, have been the better choice. We must correct for that now.
In the 1950's, the demographic structure still resembled the
pyramidical shape (with some war-related dents). Today, it
resembles a pumpkin: few children, still many actively
employed, and a rapidly growing number of retirees.
From 2001 to 2050, the share of those who are over sixty will
rise from 24 to 37 per cent in the Germanys population. (Figure
22).
Changes within the pay-as-you-go system will not be able to
reverse the trend. Furthermore, government policies have been
partly offsetting: While child support payments and subsidies
to families favour raising children, other policies are in support
of women participating in the labour force which raises the
payroll tax volume of the active generation, but also helps to
raise the average age of women when they first give birth and
reduces their desire to have (several) children. The retirement
age also can be raised to balance the books, but that will now
only partially offset the past trend towards early retirement (Figure 23).
All in all, such measures provide some relief and
buy time. They do not solve the problem. The system is on
auto-pilot towards insolvency (Figure 23)
.
After 2020, the demographic structure will come to resemble a
mushroom: A weak stem of young and actively employed,
many elderly. Around or soon after 2030, Germany will have
one pensioner per one payroll-tax paying employee. Immigration,
retirement age, labour force participation are variables that will determine whether this happens in 2028 or 2038, but they will not help us avoid the fateful outcome: That around
that time, the average payroll tax would have to equal the
average pension, unless, of course, pension benefits would be
radically cut.
The average German pension payroll tax, standing at 19.5 per
cent in 2004, would have to be raised to around 24 per cent, if
the current structures of benefits and finances are to be
preserved (Figure 25 and Figure 26) (note 53).
It is inconceivable that the actively employed of the year 2030 will be willing to pay that, as much as it is inconceivable that there will be enough jobs to support a payroll tax of that magnitude.
As a consequence various pension reforms aim to reduce the
benefits while trying to keep the payroll tax from rising above
the current level. The decline in benefits will be substantial, as
can be seen from the projections in figure 26.
Whoever wants to assure the pensioners and those soon to retire
that their pensions will be safe, must show how that can be
achieved - not just for the year 2010, but for 2020 and 2030.
Those entering the labour force today and beginning to pay
into the system, will retire around 2030. They can expect an
answer.
b. PENSION REFORM: Solution: Fully Funded Pensions and Family Values
With the generational contract defunct, we have only this alternative:
either return to the pre-20th century intra-family
"contract" under which the active generation cares for both its
own parents and children, or take care of your own retirement
by building up a capital stock for old age. We may yet see a
partial return to the seemingly outdated bondage of three
generations within a family. This will and need not take the
form of three generations living under the same roof.
In the 20th century, the societal, government-instigated
intergenerational contract has contributed to the erosion of intra-
family bonds, with the government posturing as a more
reliable guarantor than family tradition. Why should this trend
not be reversed in the 21st century, as we recognize that
building on government was building on sand? Is it not cynical
to deride compassion for those we know personally and whose
needs we can judge ourselves, while demanding anonymous
solidarity across society, with a bureaucratic entitlement
system often giving too little to the needy and too much to
those that can take care of themselves? The empowerment
reform twins effective compassion and individual
responsibility.
As un-guaranteed as the family contract has been (there never
was and will be assurance that children will be willing and able
to care for their parents), at least it builds on common values.
Ethical norms are never guaranteed, but expected to be
adhered to. While not air-tight and rock-solid, they are more
stable than the current system's house of cards.
The second, complementary or alternative, pillar of the future
old age provision will be a fully funded pension system as a
complete or at least partial replacement of the pay-as-you-go
system. Full replacement would be a gigantic task, especially in those countries where government retirement plans play the dominant role. It is only achievable if society is willing to shoulder an enormous dual burden: Those in the labour force
would have to continue to finance the pensions of both the
elderly and those soon to retire who no longer can build up a
sufficiently sized fund; and the young would have to set aside
further savings for building up their own retirement fund, so
that, eventually, the next generation would only be responsible
for itself. Even if the process would be stretched over an entire
generation, the burden is enormous. Societal consensus on such
a radical effort can probably only be reached in a situation of
severe crisis, such as in Chile in 1980.
It is seemingly paradoxical: The less bankrupt the current
system is, the less will a society be willing to change course to
avoid catastrophe. But recognition of the right path should
suffice to make at least partial provisions. Furthermore, the
success of even a partially funded pension plan will unfold
persuasive power. It is, therefore, not necessary to demand the
full replacement of the current system, reasonable as that
would be. Appetite increases with eating.
Even partial and gradual replacement of the current system by
a fully funded plan will require the current generation to save
considerably more and sacrifice consumption. The sooner we
start, the smaller this sacrifice will be, and the sooner we can
ease up. Asking for such sacrifice is not asking too much at this time.
For the first time in this century, the young generation inherits
assets that were not destroyed by a war or devalued by a
hyper-inflation, especially so in Germany. Compared with the
generation that lived through the first half of this century, this
extra and only financial burden is moderate.
Furthermore, in an inter-temporal sense there really is no extra
burden: If we keep the pay-as-you-go system, payroll taxes will skyrocket, imposing a tremendous extra mortgage on future generations. By building up a fully funded system, we discount the otherwise inevitable future burden and shoulder it, now.
Moreover, there is a net gain: The eventual bankruptcy of the
current pyramid scheme would come at the cost of social and
political upheaval. By building up a fully funded plan, the current
generations do have to shoulder an extra burden, but the
future generations will be relieved of vast financial and social
consequences. In an inter-temporal sense, this investment will
have a high return.
The current generations' extra burden can be eased by the
savings in the Social Savings Accounts. The more prudent
employees become in drawing benefits from the other areas of
sick leave, health and unemployment insurance, the less "fresh
money" they will need in building up their retirement funds.
While the empowerment model does ask the individual to get
out from underneath the welfare state's mouldy but still warm
blanket and test the breeze of individual responsibility, the SSA
balances saved from other social security areas provide the
charming comfort of a warm-up. Reforming all social security
areas offers attractive synergies.
Apart from financing an extra burden now for the sake of
preventing disaster down the road, pension reform takes the
same steps as in the other areas:
- (1) Put all current pension payroll taxes, employer- and
employee-paid, into the Social Savings Account of the
employee. Initially, this money will only be in the SSA in
transit, as it has to be paid out to the pension recipients
that can no longer build up a retirement fund (Figure 27).
At the same time, individuals will be asked to gradually
build up a fully funded plan. This can be sped up, if we
decide to allow individuals to use part of their current payroll tax for that purpose, and cover the shortfall in current pension outlays out of the government budget. If
compensating budget cuts are unavailable and a tax increase
is unavoidable, raising the value added tax would
be least harmful, as this tax on consumption favours
savings, savings which we need for additional voluntary
contributions into the new funded pension system. In
addition, exempting these voluntary contributions from
income tax would favour saving still more (note 54).
(2) As the claims under the pay-as-you-go system decline with
retirees passing away, more and more of the payroll tax
can be steered towards the fully funded plan.
Back to contents
VI. CONCLUSION
Individual Responsibility and Effective Compassion
Reforming the welfare state is inevitable if we want to preserve
social security: Without reform, the social systems would collapse.
But we need not take an axe to benefits. A marketoriented
reform whose cornerstone is individual responsibility
need not be bloody.
With the empowerment reform, we get rid of the welfare state's
top-down entitlement system. In the new social state, we let
individual responsibility first start-up, then drive the system.
Effective compassion takes the place of solidarity.
The reform puts the individual where he belongs: at centre
stage. He is both enabled and made responsible to make decisions.
The call for efficiency and individual responsibility
cannot be criticized as coming from a cold heart disregarding
individual needs. By first financially empowering the
individual to finance his choice, the no-loss rule is preserved.
With the dual emphasis on individual empowerment and
responsibility, the call for efficiency, often perceived as
abstract, assumes a tangible, personal meaning: Individual
purchasing power to buy current benefits, individual
appropriation of savings resulting from voluntary restraint. Second,
the consequences of poor choices are mitigated, since
mandatory coverage levels provide a safety net. We provide a
road system, traffic rules, guard rails, but do not dictate the
choice of car vs. bus. We do prevent people from driving off
the cliff.
The Social Savings Account can be applied to all of the four
areas dealt with here - sick leave, health, unemployment,
pension. That is a major advantage. Substitution within each
area as well as between them - savings from unemployment
insurance used for pension insurance - is not just possible, but 75
desirable, a feature that unfolds particular benefits for the
gargantuan task of pension reform. Everyone can compose his
social security menu according to his needs, with a minimum
level being mandatory, but the provider being always the
individual's to choose.
Inasmuch as the current beneficiaries, mostly employees, can
only gain under this proposal, one might question why the noloss
rule should be so strictly applied. If employees' sick leaves
will decline, if they opt for lower unemployment
compensation, would it not be better to share some of their
premium savings with their employers? Labour cost would
decline faster, job growth would be higher, the financial base
for the social system would broaden - a win-win situation for
employers and employees. We leave that decision to employees
and employers and hope that such common sense will prevail.
What we wanted to show is that, even when employees should
refuse such concessions, the system can be successfully reformed.
Employers, remember, would also gain, even when they fully
transfer their current cost or payroll tax share into the SSA's of
the employees. In the past, these components of indirect labour
cost have risen much faster than direct wages. With their
transfer into the SSA, they become part of direct wages and, in
the future, rise only in step with them.
In regard to the no-loss rule it is also legitimate to question
why all the current cross-subsidies should be sacrosanct: Why
should it be written in stone that even well-off pensioners
should have their health care expenses subsidized by the
actively employed? Why should those that have foregone
income while being trained carry part of the unemployment
cost of the unskilled that have spurned training? Why should
single and dual income households subsidize the health costs
of middle-income families?
Today, all of these subsidies are being justified in the name of
solidarity. Whoever questions them is reprimanded as lacking
compassion. But does compassion demand even middle-class
income transfers, which amount to a regressive tax?
We remain mute on this question - not for lack of personal opinion,
but because this judgment is society's to make. And it will
do so. When enacted, this proposal will open the Pandora's box
of debate on these subsidies. Once the currently hidden income
transfers are made explicit and individually transparent on
everybody's Social Savings Account, the curtain on this debate
will open. Few people in Germany, for example, are currently
aware that more than half of the health payroll tax goes
towards such transfers. Information on who and how much is
subsidized is an important side-effect of this reform. Full information
is a pre-condition for a sound democratic debate. We
must not keep the veil over these data.
Whatever the outcome of this debate, whether there is an
outcry over these transfers or whether they are confirmed, the
meaning of solidarity will no longer be abstract, unrelated to
the knowledge of who receives what and whether he deserves
it. Solidarity will regain the meaning that it has lost in the wake
of the welfare state: people's intentioned and informed
compassion for each other.
Simple, Radical, Social.
The proposed empowerment reform does not slash the social
safety net. While it is radical in the sense of a root-change -
abolishing the welfare state -, it neither axes benefits nor
institutions. It allows the individual to evolve from passive
beneficiary of entitlements into an active and sovereign
consumer of social insurance products. A society of free and
mature individuals does not treat its citizens as wards. And the
empowerment reform also allows the current entitlement
bureaucracies to evolve into efficient, client-driven providers.
The empowerment reform is social in the sense of adhering to
the no-loss rule. Nobody loses except for those that abuse the
system and contribute to efficiency losses. The quality of social
security is, at the minimum, preserved. Its cost goes down.
The empowerment reform is simple, because it can be financed,
because it can build on current institutions and, above all,
because it builds on people's ability to decide responsibly while
also, as a back-stop, having a safeguard against individual
errors.
When neither employees, employers nor society lose, and if
each party senses more pleasure over its own than envy over
the other's gain, then this reform should be a self-starter.
Simple, unfortunately, is not easy. As Ronald Reagan
remarked: "The experts tell us there are no simple answers to
our difficulties. They are wrong. There are simple answers, just
not easy ones."
Yes, empowerment reform is difficult. It faces the powerful
opposition of the paternalistic guardians of the welfare state,
whose status would melt like snow in spring once we are empowered
to act with self-responsibility. We have accepted this
custodial structure for too long; the welfare state has corrupted
our minds, many of us having become insecure, doubting that
we can decide for ourselves. Building self-confidence towards
individual responsibility is the most difficult task. And it is
worth the effort.
Back to contents
ENDNOTES
1: Want, disease, ignorance, squalor, and idleness.
2: The no-loss rule cannot be claimed by those that abuse the
system.
3 Christoph Schroder: Industrielle Arbeitskosten im
internationalen Vergleich. In: iw-trends 3/2003, Cologne, p. 10.
4 Institut der deutschen Wirtschaft (IW): Deutschland in Zahlen,
various annual editions. For 2002, the Institut der deutschen
Wirtschaft reports 77.9 percent, compared with 77.4 per cent in
2001. Differences in the data presented in the table are based on
changes in the calculation method. Institut der deutschen
Wirtschaft (IW): Personalzusatzkosten in der Deutschen
Wirtschaft. In: iw-trends 3/2003.
5 OECD: Taxing Wages: Income Tax, Social Security Contributions
and Cash Family Benefits 2001-2002. Paris, 2003, p. 16 and own
calculations.
6 If the pension benefits would not be lowered (as they have been
by several measures between 2000 and 2004).
7 The German public health system's mandatory sickness funds -
Gesetzliche Krankenkassen - could be more aptly named "kranke
Gesetzeskassen" - sick mandatory funds.
8 For an authoritative work on consumer-driven health care, see
Regina Herzlinger: Market-Driven Health Care, Perseus Books,
Cambridge, Mass. 1997.
9 In the case of unemployment insurance, similar subsidization
takes place, where unemployment compensation is linked to
family size and net income, while the payroll tax is based on
gross income. And the pension system gives credit for time spent
in the military or unemployment, among others, and does not
make full actuarial deductions for early retirement. The pension
system also gives credit for time spent in higher education or for
rearing children. But these credits can be justified. In a pay-asyou-
go system, children will pay the current generation's
pensions, and higher income earners pay a higher payroll tax.
10 The mandatory minimum level can also be made dependent on
income.
11 This restriction can, of course, be relaxed, if a substantial sum has
been accumulated in the SSA. However, withdrawal for
consumption purposes would require that the amount is first
subjected to income taxation, since the deposits had been tax-free.
12 The range of investments that SSA balances can be used for can
also be made dependent on the size of SSA balances. As the SSA
is built up, more illiquid and higher risk investments can be considered.
13 If the balances would not go to the holder's estate, incentives to
save them would be diminished, especially in old age;
furthermore, while there should, in general, not be any
inheritance tax, exempting at least SSA balances from inheritance
taxes should be a given, since the future generation needs this
capital for its own social security, especially in the long transition
phase needed to build up a fully funded pension plan.
14 Bundesministerium fur Gesundheit und Soziale Sicherung:
Gesetzliche Krankenversicherung . Personal und
Verwaltungskosten 2002. Berlin 2003, p. 7 and 10.
15 To qualify for an HSA, the consumer must opt for a highdeductible
plan with a minimum deductible of $1,000 for
individuals and $2,000 for family coverage. For 2004, the consumer can then invest, tax-free, up to $2,600 (individuals) and $5,150 (families) into the HSA as long as the deductible is at least that high. Withdrawals from the HSA can be made tax-free for
medical expenses. After age 65, money can also be withdrawn for
any purpose and is subject to income tax. Therefore, the HSA
extends beyond health and becomes a retirement account. Much
credit for developing and promoting consumer-driven plans and
savings account concepts is owed to market-oriented think tanks,
in particular John C. Goodman of the National Center for Policy
Analysis, www.ncpa.org, Greg Scandlen and Grace-Marie Turner
of the Galen Institute, www.galen.org, Joseph Antos and Robert
Helms of the American Enterprise Institute, www.aei.org, Stuart
Butler and Robert Moffit of the Heritage Foundation,
www.heritage.org.
16 Michael Rothschild, Why Health Care Reform Died, Wall Street
Journal, September 22, 1994.
17 The rates pertain to 2003. Missoc . Mutual Information System on
Social Protection in the EU Member States and the EEA, 2003.
18 Rigmar Osterkamp: Work Lost Due to Illness - An International
Comparison. Cesifo Forum 4/2002, p. 37.
19 Christoph Schroder: Personalzusatzkosten in der deutschen
Wirtschaft. iw-trends 2/2003, p. 11.
20 Sick leaves also fluctuate relative to job risks. They tend to be
lower in recessions, further proof that health conditions are not
the primary cause of variations in sick leaves.
21 In keeping with the no-loss rule, the maximum pay-out has to be
the firm-specific cost. Companies with sick leave expenses lower
than the average would be penalized if they paid out on the basis
of the industry average.
22 Unemployment compensation, by definition, precludes a drop to
welfare levels.
23 Rigmar Osterkamp: Work Lost Due to Illness - An International
Comparison. Cesifo Forum 4/2002, p. 39
24 Nordiske Arbeidsgiverforeninger 2004.
25 In October 1996, sick leave payments, which have to be paid by
employers, had been reduced to a legal minimum of 80 per cent .
instead of 100 per cent . of income, although all labour contracts
kept calling for 100 per cent. After the Social Democrats had won
the 1998 elections, the mandatory sick leave payments were
increased again to 100 per cent of income in 1999.
26 In Germany, total sick leave costs are estimated to be 71 billion
Euro, or respectively, 3.44 per cent of GDP (Bundesanstalt fur
Arbeitsschutz und Arbeitsmedizin. Kosten durch
Arbeitsunfahigkeit 2001). According to the German employers'
association, companies alone have to pay about 37 billion Euro
for outright wage / salary compensation (BDA: Strukturen und
Entwicklungen bei krankeitsbedingten Fehlzeiten. In: Soziale
Selbstverwaltung, February 2004, p. 10 f.).
27 BDA: Strukturen und Entwicklungen bei krankheitsbedingten
Fehlzeiten. In: Soziale Selbstverwaltung, February 2004, p. 11.
28 Statistisches Bundesamt: Index der tariflichen Monatsgehalter.
29 In public health insurance in West Germany, the share of
administrative costs to total expenditures increased from 4.3 per
cent in 1980 to 5.5 per cent in 2002 (Institut der deutschen
Wirtschaft (IW): Deutschland in Zahlen 2003. Cologne 2003, p. 77.
30 A health maintenance organization (HMO) can be defined as a
pre-paid service plan: Delivery of care and insurance are integrated. There is a fixed per-capita-fee per year/month irrespective of use of care. All use of the HMO's services are paid
for by this capitated fee.
31 The rates pertain to 2003. Missoc . Mutual Information System on
Social Protection in the EU Member States and the EEA, 2003.
32 In most Bismarckian countries (e.g. Germany, Greece,
Luxembourg, Netherlands, Spain), there is an upper limit to the
income subject to the payroll tax - in Germany's case and for
2004, the limit is at . 61,800 p.a. in case of pension and
unemployment insurance, . 41.850 in case of health and nursing
care insurance.
33 Of course, any single one of these characteristics does not suffice
to make the payroll tax exceed the full actuarial value of benefits.
34 Until 1983, pensioners did not contribute at all; until 1989, they
contributed at half of the payroll tax rate, and since 1989, at the
full payroll tax rate. For pensioners, since they are no longer
employed, there is no employer's share. As of April 2002,
however, the full payroll tax is also assessed on pensions from
company plans. This will increase the pensioners' share in the
middle bar of Figure 17).
35 In contrast to U.S. Medicare, there is no fund for old age reserves
from which at least part of the medical expenses of the elderly are
paid.
36 In the transition from the old to the new system, an insurer or
provider must not deny coverage to somebody with a preexisting
condition or charge a higher premium. Correspondingly, the noloss
rule dictates that a provider's losses from having to take on
such bad risks would be recouped from slightly higher than
actuarially calculated premiums charged to the vast majority. If,
in the future, a good risk develops into a bad one, this poses no
problem, as this is the nature of insurance. Also, free choice of providers must not be restricted to the first time of signing up,
since otherwise a beneficiary would be locked in as he gets old.
To allow for switching from one provider to another one at any
time, providers must build up actuarially adequate old-age
funds, since health expenses rise with age. The old-age fund must
be vested in the beneficiary and thus be portable if he decides to
switch to another provider. Since the current system does not
have an old-age fund, building it up requires extra money to be
spent now, i.e., a mark-up on the premium that reflects current
actuarial benefits. In an intertemporal evaluation, however, this is
not an added cost, since an old age fund would assure that the
premium does not rise with age, in contrast to the age burden
that we will have to expect under the current generational
contract and our demographic trends.
37 As noted before, the distinction to medical savings accounts as
applied in the U.S. is that unspent balances cannot, at year end,
be withdrawn for just any spending, a vacation or other
consumption spending. The reason is that the SSA encompasses
all of social security.
38 This example underlines that reforming both sick-leave and
health policies entails synergies.
39 In Germany, the administrative cost of the public health system
amounts to 5,6 per cent of expenditures, or over 8 billion Euro in
2002, or 157 Euro per insured and year. (Bundesministerium fur
Gesundheit und Soziale Sicherheit: Endgultige
Rechnungsergebnisse der gesetzlichen Krankenversicherung
nach der Statistik KJ 1 . 2002. Bonn 2003, p. 116 and 225.)
40 A hospital catering to patients of the sickness funds . which
encompass 90 per cent of the population - has to obtain a state
permit which imposes a ceiling on the number of beds etc.,
accompanied by a state commitment to pay for investment cost.
With an excess supply of hospital beds, state consent to build or
expand a hospital is difficult to obtain; and many communities
are opposed to privatising their hospitals out of fear that they lose "control", although these hospitals typically require subsidies.
41 In physician practice-management companies, doctors do not
operate independent practices, but belong, with their practice, to
a tightly organized company. Economies of scale in purchasing
supplies, effective use of equipment and savings of overhead can
lower costs.
42 Bundesministerium fur Gesundheit und Soziale Sicherung:
Gesetzliche Krankenversicherung . Personal und
Verwaltungskosten 2002. Berlin 2003, p. 113.
43 DRG = Diagnosis Related Groups.
44 The rates pertain to 2003. Missoc . Mutual Information System on
Social Protection in the EU Member States and the EEA, 2003.
45 Bundesanstalt fur Arbeit: Strukturanalyse . Zu- und Abgange an
Arbeitslosen im Juni 2003 . Vorlaufige Ergebnisse. Nurnberg,
2003, p. 3.
46 This only holds for lower or medium incomes, since there is a cap
on unemployment compensation as well as on the income that is
subject to the payroll tax.
47 35.4 per cent in 2002.
48 Alexander Reinberg, Markus Hummel: Geringqualifizierte . In
der Krise verdrangt, sogar im Boom vergessen. In: IAB
Kurzbericht, Nr. 19 / 2003, p. 4.
49 Enthusiastic support for vocational training cannot be
interpreted, as others might do, that training is a cure-all for
unemployment. If it were, German unemployment would not be as high as it is. Vocational training can mitigate, but not outweigh the labour cost disadvantage of Germany.
50 A premium at full actuarial value would then mean that the
unskilled would pay a higher premium than currently, if they
sought current benefits; this would violate our no-loss rule.
Therefore, the premium discount for those seeking training could
be phased in gradually.
51 Bundesagentur fur Arbeit: Quartalsbericht der Bundesagentur fur
Arbeit - Bericht uber das vierte Quartal und Kurzbericht zum
Geschaftsjahr 2003. Nurnberg 2004, p. 5 and 12.
52 Germany's public pension system has no fund at all, and its
liquidity reserves are hovering around zero, not even covering
one month. Other countriesf pay-as-you-go-systems do not fare
much better.
53 Nachhaltigkeit in der Finanzierung der Sozialen
Sicherungssysteme - Bericht der Kommission unter dem
Vorsitzenden Bert Rurup, Berlin 2003, p. 99.
54 Such tax exemption could be criticized as endangering efforts to
balance the budget. An alternative would be to pay contributions
out of after-tax income, but exempt the interest from taxation.
This tax loss on future interest is outweighed or at least partially
compensated by the growth-enhancing effect of these savings.
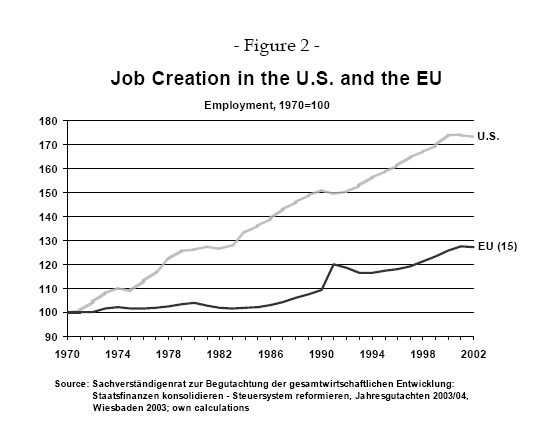{kind=link}
{kind=link}
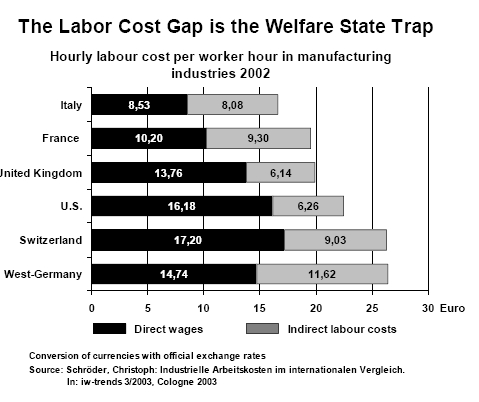{kind=link}
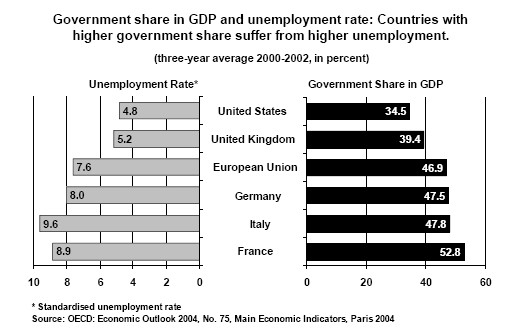{kind=link}
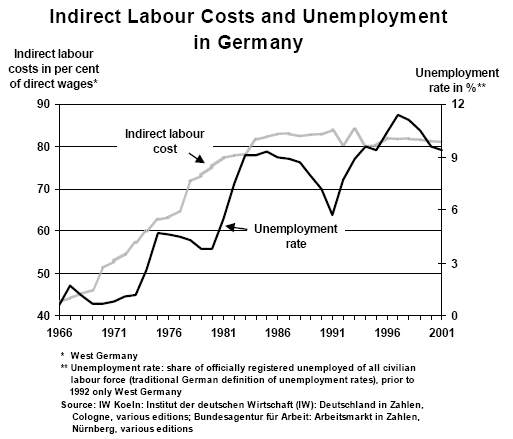{kind=link}
{kind=link}
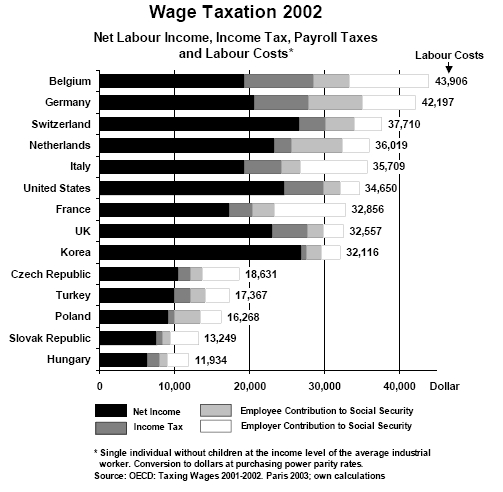{kind=link}
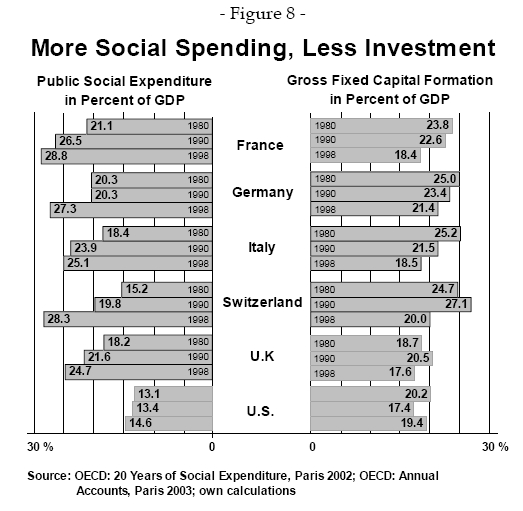{kind=link}
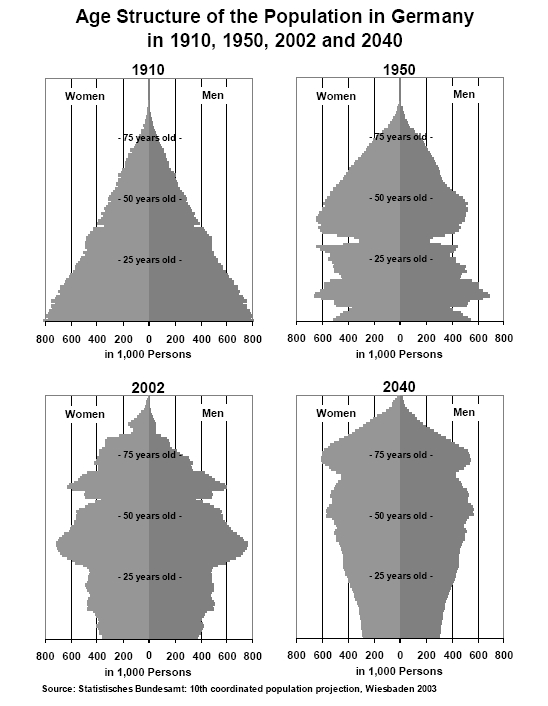{kind=link}
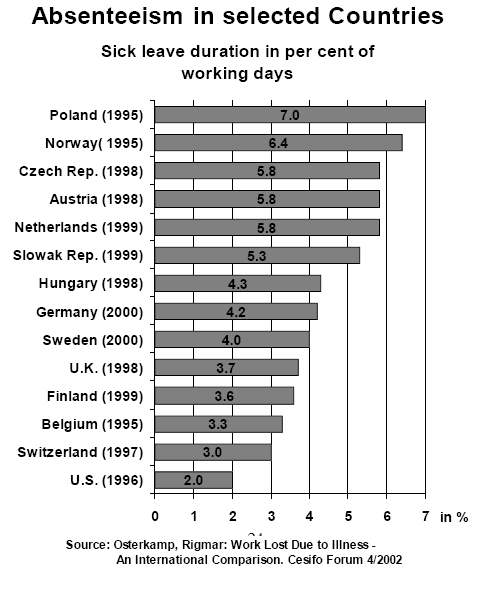{kind=link}
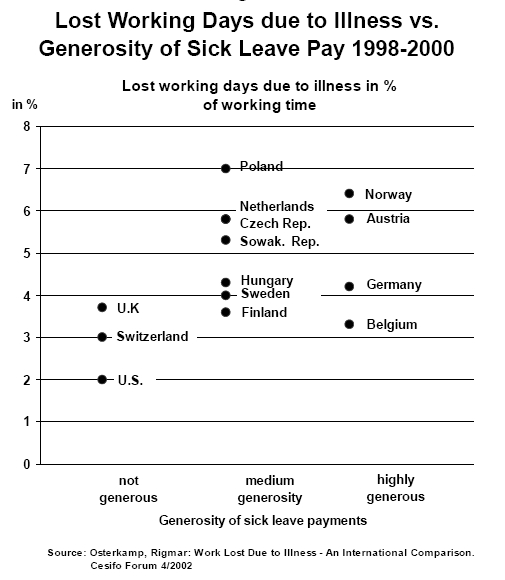{kind=link}
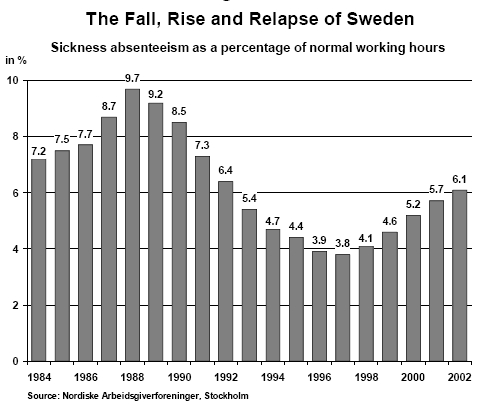{kind=link}
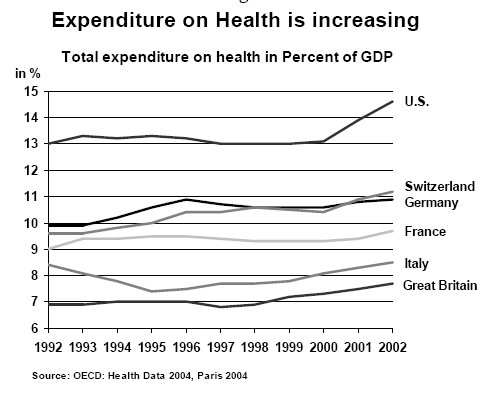{kind=link}
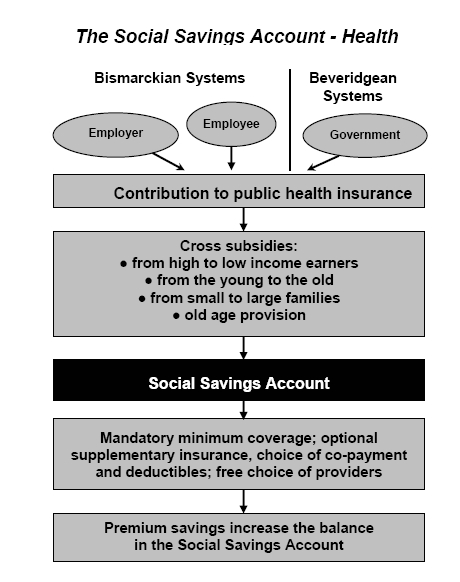{kind=link}
{kind=link}
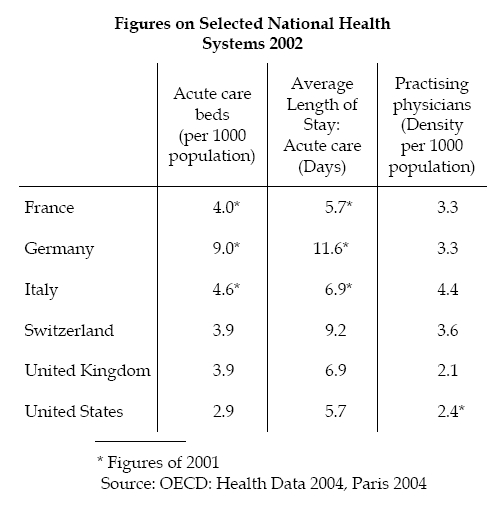{kind=link}
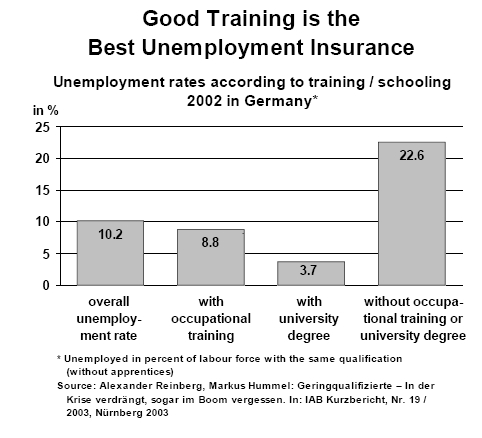{kind=link}
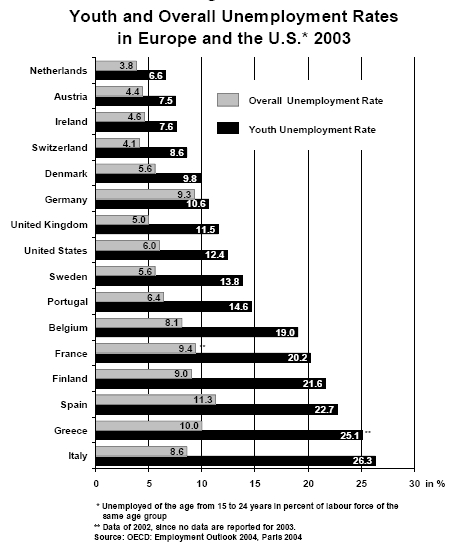{kind=link}
{kind=link}
{kind=link}
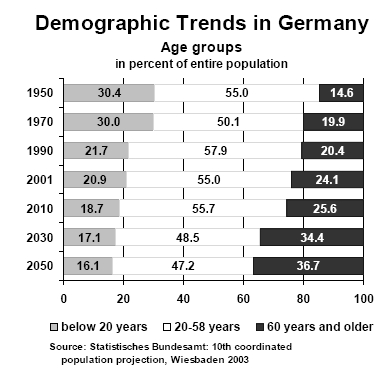{kind=link}
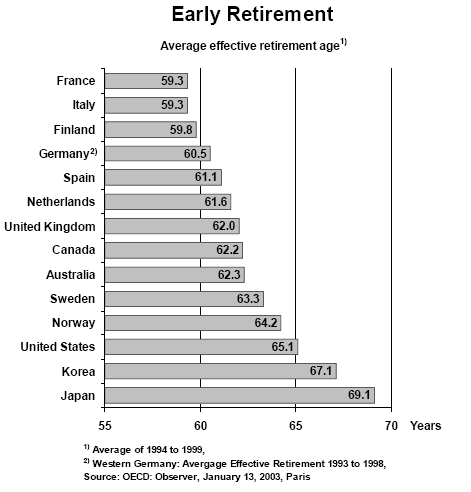{kind=link}
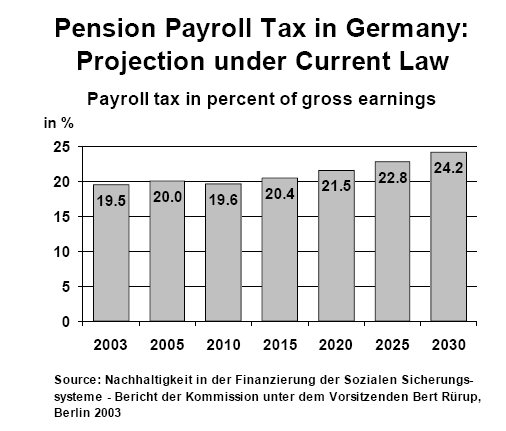{kind=link}
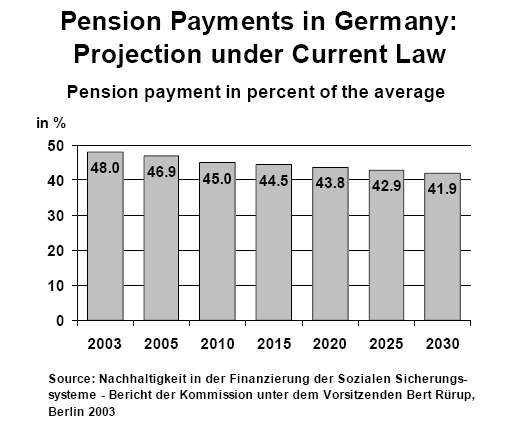{kind=link}
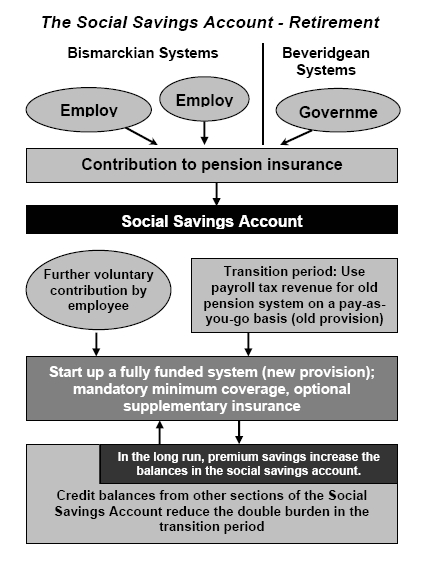{kind=link}